In 2014, my youngest children and I attended a family-friendly party in a sprawling yard where I had a long conversation with a smart and funny woman my age. Nearby, my nearly 2-year-old daughter, Lyra, moved remarkably fast using her newly perfected bear walk.
“She’s so cute, how she crawls on her hands and feet,” the woman said.
“Yeah, it takes children with Down syndrome longer to crawl and walk.”
“Wait, your daughter has Down syndrome?”
“Oh, yes,” I said.
“You are so much stronger than I could have been,” she said, but I disagreed.
“No,” she continued, “I’m telling you that you are stronger than I was. In my late 30s, I was still single and had IVF to get pregnant. When I was pretty far along, they told me the baby had Down syndrome and gave me two days to decide. I couldn’t do it. I would have been alone, I … I didn’t do it.”
“I have no judgment,” I said, knowing this woman made the best decision she could with the information she was given. The features on her face rearranged themselves, her eyes going from narrowed and intense to widely opened.
“But I see your daughter and,” she paused, “it makes me wonder…”
I was reminded of that conversation when I recently learned of a YouTube influencer and his wife who decided to terminate her planned pregnancy. Until then, I had never heard of Jesse Ridgway, whose story-telling videos have earned him over 4 million followers.
Weeks earlier, the Ridgways had shared with the public the exciting news of their pregnancy. Then, on June 3, Ridgway posted on his X account that his wife had undergone an abortion because of a fetal DS diagnosis. Rather than simply asking for privacy and compassion, Ridgway felt the need to justify why they had chosen to end the pregnancy, describing what he believes living with DS to be like, not only for people with the syndrome, but also their families. His post contains both misleading and patently false information, as well as his assessment that “Down Syndome isn’t a ‘blessing’, it is objectively shitty from a health perspective.”
Over a decade ago, I began making an automatic monthly donation to Down Syndrome Diagnosis Network, a non-profit with the primary mission of educating health care professionals on how to give accurate, up-to-date information on Down syndrome at the time of diagnosis. Unfortunately, as Ridgway’s post underscores, the work of the network is far from over.
In his post, Ridgway states the odds of having a baby with DS are 1 in 1,000, which is true if the mother is 28. But at 31, Ashley Ridgway’s chances of having a baby with DS were 1 in 800. When I was pregnant with my daughter at 45, my odds were 1 in 30. For a 20-year-old, it is 1 in 2,000.
Choosing to bring a child into the world always includes the gamble of a diagnosis. But unlike other diagnoses, such as autism spectrum disorder, ADHD, eating disorders, childhood cancer, depression, bi-polar disorder, addiction and many more, DS can be definitively diagnosed prenatally because it is caused by the observable presence of an extra twenty-first chromosome.
Are there challenges raising a child with DS? Of course there are, as there are with any child.
As for health concerns, Ridgway is correct that roughly 50% of newborns with DS are born with heart conditions, the most common of which is atrioventricular septal defect (AVSD). But in the past 40 years, tremendous advances in cardiac care have occurred and, according to the National Institutes of Health, over 95% of newborn AVSD surgeries are successful, including for babies with DS.
Ridgway also mentions hearing challenges and vision problems, yet that is not the same as deafness and blindness. Many hearing problems people with DS have are treatable conditions, such as “glue ear” in which secretions accumulate in the middle ear, something simply solved by regular monitoring and cleaning when needed. Similarly, the majority of vision problems in Down syndrome are the same as those in the typical population: nearsightedness, farsightedness and astigmatism − all of which are easily corrected.
But of all the misleading statements Ridgway made, the most egregiously false is: “I didn’t realize just how rough it is for the child, let alone the family…”
Dr. Brian Skotko, a Northeast Ohio native who is now the director of the Down Syndrome Program at Mass General Brigham in Boston, has conducted several studies on the quality of life for people with DS and their families. He found that “nearly 99 percent of people with DS indicated that they were happy with their lives, 97 percent liked who they are, and 96 percent liked how they look.” He also surveyed siblings of people with DS and 88% said that they are better people for having had a brother or sister with DS. That finding was surely no surprise to Skotko, who has a sister with DS.
Lyra and Leif, 2014.Viking siblings swim at Lake Charlevoix, 2023.Lyra gets in on her brothers Leif and Hugo checking who’s taller, 2024.Leif and Lyra sledding, 2026. Lyra loves both sledding and downhill skiing.
As for parents, a National Institutes of Health study found the divorce rate for couples with a child with DS is lower than in families that have a child with a different birth diagnosis and also lower for those with children that have no identified disability.
I respect the Ridgways’ decision to terminate a wanted pregnancy in the face of a DS diagnosis, just as I respected the choice of the woman I met 12 years ago. But I call him out, particularly as someone whose job is literally to influence people, for using his experience to promote the bigotry of ableism − the belief that those among us without certain IQs, abilities and incomes are strictly a burden, not valued members of society. As with any bigotry or bias − which are always based upon falsehoods− getting to know someone seemingly unlike you often leads to the discovery they are not so different after all.
This column was first published in the Akron Beacon Journal on Sunday, June 21, 2026.
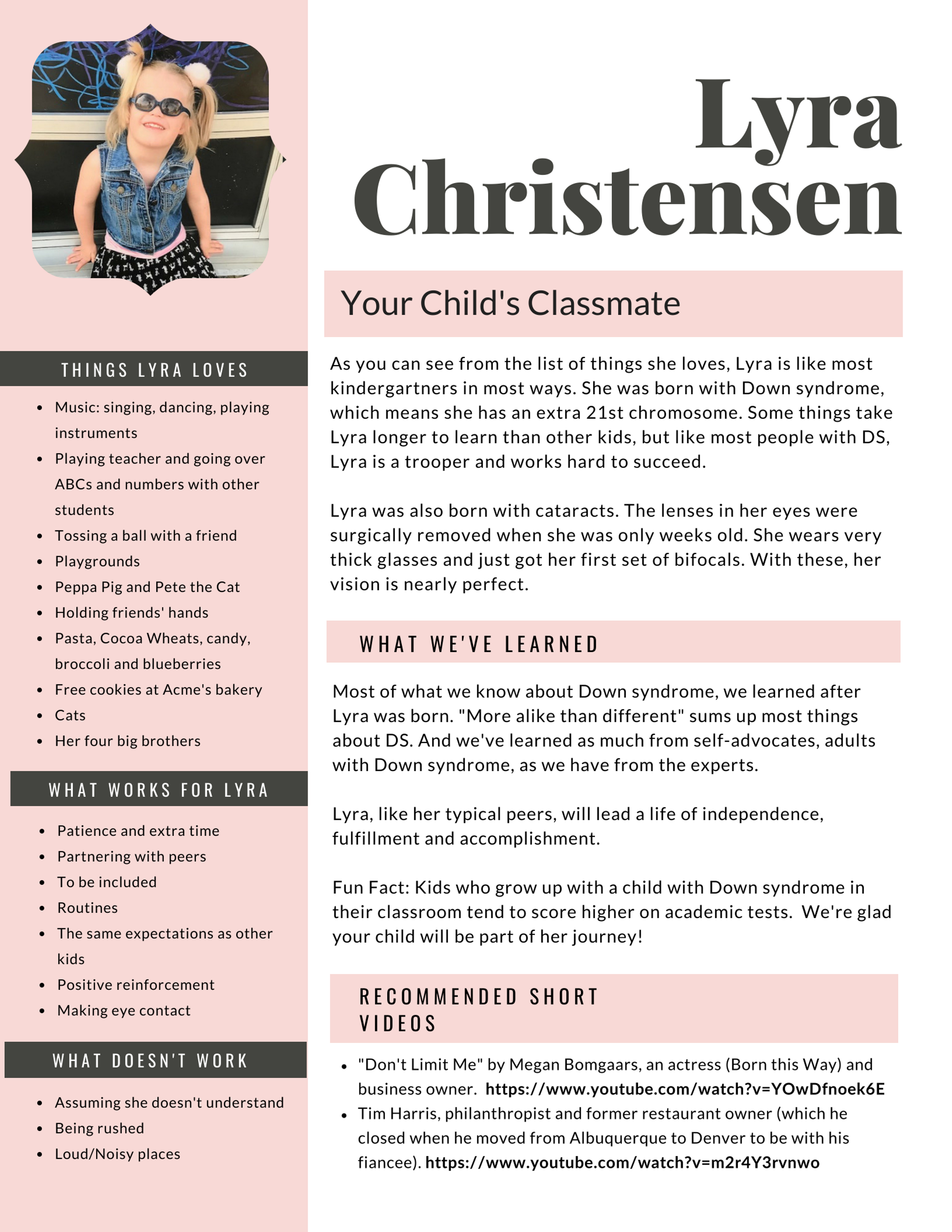
Many families make flyers to send home with the classmates of their children with Down syndrome. I’ve seen several made by friends of ours, who helped us with ours.
Rather than wondering if Lyra has Down syndrome or why one student in the classroom receives extra assistance, a flyer gets in front of the proverbial bus. Information can dispel misunderstanding and fear and encourage acceptance.
Tomorrow is Lyra’s first day of kindergarten. She will be fully included in a general ed classroom with “push-ins” (assistants come into her classroom rather than pulling her out). There is not a single study that shows improvement for students who are in segregated classrooms based upon disability.
Furthermore, not only do typical students who grow up with a classmate with an intellectual disability become normalized to diversity, they, too, also benefit academically from inclusion.
The first two years with a baby with Down syndrome are a lot of work, but then it all gets easier.
I have repeated that sentence, spoken by the caseworker from our county’s DD Board when Lyra was only a few months old, many times over in my thoughts. Lyra turned two years old in August of last year, and for the past six months, I have considered where Lyra is now, and also how our family has transitioned and developed with this fifth child, our only daughter who has Down syndrome.
Yet I have struggled in my attempts to write about this pivotal place where we find ourselves after long anticipation. Two months ago, I wrote “Two Years This Family” intending to immediately follow that essay with “Two Years This Daughter.” And I tried, writing two lengthy drafts that I promptly shelved. Instead, I found more enjoyment writing other pieces, which are also about Lyra, the reality of Down syndrome today and how our society, by in large, remains misguided in its understanding and treatment of people with Down syndrome. Those essays, like all my writing, did not come easily, but were the products of days spent at my desk, writing and re-writing until my brain, as it does after a long day of writing, would buzz like a nest of agitated hornets. That’s when I know to step away from my computer, consider a shower and head out for a long hike. A missing sentence or section or elusive phrasing will sift up, time and again, when I am deep in the woods, breathing hard as I hike up the hills of a two-mile trail in the metropark near our house, not concentrating, but lightly holding the piece of writing, as though it were floating like a cartoonist’s thought bubble, just above my head. It was good, hard work, resulting in essays that I submitted for publication rather than post on Whoopsie Piggle.
The problem with my previous attempts to write about Lyra at the age of two is the essays were boring to write and, thus, boring to read. It is my job, as a writer, to make the material engaging. But describing therapy sessions that began, in the case of speech, when Lyra was a few months old became a dry litany in my hands: we did this, and then this, and some more of this with a little added that, until here we are today, still doing some of the same, but not all the same and trying out some other things as well. Let’s skip the process for now and get to the results:
Lyra walks and
She talks and
She feeds herself and
She plays with toys, but more often disappears in the house and takes everything out of any cupboard, dresser drawer or laundry basket she finds within her reach that has been left unsecured. “I see it has been raining baby clothes,” Max says after Lyra has shoved, yet again, several of her shirts or Leif’s pants through the railings of the balustrade on the second floor of our home. Clean clothes purloined from the dressers in the adjacent bedrooms only to be flung onto carpeting coated in cat hair. Thanks, kids.
Yes, Lyra’s acquisition of early childhood milestones came later than for most typical children. But not all that much later and now, at two and a half, Lyra is pretty much like any two-year-old.
The difference lies less with our daughter than with us, which is what Lyra’s caseworker meant by “a lot of work.” Before Lyra, I had never broken down the mechanics of a baby learning to hold up her head, sit up, crawl or walk (gross motor skills). Neither had I considered that my babies picked things up by first using their fingers as rakes and later developing a precision pincer grip with their forefingers and thumbs (fine motor skills). Nor had I worked to train a baby’s tongue to move into the mouth and not rest on his lips (important for speech). I know how to drive a car even though I don’t know the first thing about the mechanics of automobiles. Similarly, I have long understood how to raise small children but my focus was on behavior and education, not how their little bodies went from infant blobs to motoring and motor-mouthed toddlers. They took care of that part of development themselves.
This begs the question, for me at least, how would Lyra have developed without interventions? I have no doubt that she would have learned to sit up, crawl and walk, but perhaps later. More importantly, I believe many of the interventions have helped Lyra learn how to move and use her body correctly, minimizing any overcompensation for her low muscle tone, or hypotonia, a hallmark complication of Down syndrome. And as a socially extroverted child, there is no question Lyra would be talking even if she had not had any speech therapy. However, she would be harder to understand. That is because we have spent over two years helping strengthen Lyra’s tongue and train it to stay, for the most part, in her mouth. The importance of tongue placement for speech was explained to us by Talk Tools founder and speech therapist, Sara Rosenfeld-Johnson, at the 2013 National Down Syndrome Congress convention. She told the audience to sit back in their chairs and lift up both legs so that they were parallel to the floor. She then asked us to move our legs, in tandem, from side to side, around in circles, up and down. After that, she asked us to scoot forward on our seats and try to do the same thing with our legs. What was simple when sitting back was nearly impossible when sitting on the edge of our seats. The same is true with tongues and speech. When positioned on the lips, a tongue is far harder to control and speech less precise than when a tongue is positioned inside the mouth.
There are many subtopics and nuances to Lyra’s interventions, such as the significance of music in Lyra’s learning or long-term breast feeding, that are important, sure, but those are perhaps best described in separate essays.
I wish I had worried less about the person my child would become and just enjoyed the baby she was.
I also regularly think of this quote, which I included in the essay, “Learning About Lyra,” more than two years ago. When I first read those words, just weeks after Lyra’s birth, in a book about children with Down syndrome, I knew I should do just that—stop worrying. And I also knew I could not. I had never had a child with Down syndrome. Before Lyra, I knew only one other child with Down syndrome, the daughter of an acquaintance, whom I met once, when she was a baby. After Lyra’s birth, I began to meet other families in the area through our local support group, The Upside of Downs. But equally as helpful has been a closed Facebook group for mothers of children with Down syndrome who were born the same year as Lyra. These support groups helped in the early days as we learned what we could expect for our daughter both immediately and as an adult. Yet I would be lying if I said I have not found myself, on occasion, comparing Lyra to other babies with Down syndrome who acquired developmental milestones before she did.
It turns out what has most helped me to stop worrying about Lyra is Lyra herself. As she moved out of infancy, her personality revealed itself, as any baby’s does. She’s an outgoing, curious child who loves music, dogs, cats and her brothers. Five-year-old Leif now complains that Lyra tackles him and all too often Lyra yells when he pries toys or cookies out of her hands. It’s no different than the way my first two children interacted when they were five and two.
Lyra, my youngest child, is my girl. And she’s Max’s girl. She’s her brothers’ sister and a friend to her mates at daycare. Two years after her birth, all that Lyra is has normalized. Her Down syndrome, her aphakia and contact lenses are no longer novel to us. Just as having a fifth child who is a daughter (a daughter!) has become routine. (Okay, so maybe the daughter part still tickles me like getting a long-desired present.) The point is we are a family of seven, each of us having different personalities and abilities. Claude, who is quiet and steady except when he’s excited, now writes fiction with content more intense than expected from someone so young. Hugo is confident, if not self-absorbed, demonstrably affectionate and sings like an angel. Jules, whose name means youthful, has the oldest soul of us all. He cares for everyone and everything while quietly carrying deep hurts and anger. Leif is like Hugo: bombastic, demanding and sharp-witted. Max, with his implacable patience, may have missed out on the thing he does so well, being a dad, had we not tumbled into his life when he was in his early forties. And I, who spent much of my childhood alone and lonely, never lack for company. Or love. (Could we queue in a little Sister Sledge here, please? You know the tune.)
Sarah and I were in Pittsburgh for Quilt Market where we stayed at the downtown Westin. When the elevator stopped on our floor there was a man dressed in business attire already on it. I looked over at him and could see tears welling in his eyes. By the time we got to the second floor to get off, the tears were rolling down his checks. My first impression was maybe he just got fired from his job. Then I thought maybe he was in town for a funeral. As Sarah and I walked off, he came over to us and asked if he could share something. He could barely get the words out but managed to tell me that he and his wife had been expecting their fourth child, a girl, and they knew she had Down syndrome but his wife miscarried three weeks ago. My natural reaction was to give him a hug and tell him how sorry I was. His reply brought tears to my eyes, too. He said, “Thank you for saying that. Everyone else is telling us it was the best thing that could have happened. I see your daughter and she is beautiful.” I was at a loss for words so I gave him another hug and then we went our separate ways. But I thought about that interaction all weekend. Why are people so afraid of Down syndrome that they would tell a grieving family it was for the best? ~A post in my Facebook feed this past spring.
My essays on Whoopsie Piggle have, by design, emphasized how having a child with Down syndrome is little different than having a child without Down syndrome, which is also why not all my essays focus exclusively on my daughter Lyra and her DS. I read somewhere that we are all on the path of disability whether caused by age, illness, accident or an extra chromosome. Tangentially, I have discussed medical issues that are more common in people who have Down syndrome, most particularly vision issues as Lyra was born with bilateral cataracts (occurring in 3% of newborns who have DS versus .03% of those born with 46 chromosomes). More recently, and painfully, I have written about the congenital heart problems that affect approximately 40% of the population with Down syndrome. Before this summer, I had met so many babies and young children who had undergone successful heart surgeries that I unintentionally dismissed the gravity of these cardiovascular diagnoses. And then three babies, all the same age as Lyra, died in just one week this past June. I wrote about babies Ryder, Fiona and Annie in “A Painful Week in the Down Syndrome Community.” Without rescinding my position that having a child with Down syndrome is little different than having a child without DS, I believe it is vital to discuss the possible medical complications that can accompany a diagnosis of Down syndrome. Why? Because uninformed fear causes people to say hurtful things. Because poorly informed medical personnel say fear-driven, and largely inaccurate, things when giving an expectant mother the news that the child she is carrying has an extra twenty-first chromosome. Because in some parts of the world, including regions in the United States and Canada, the Down syndrome population is undergoing a quiet campaign of genocide.
Children May Die
In my last essay, I wrote about traveling in Spain this summer with my oldest son, Claude. Watching my firstborn become a fully-fledged adult has made me ridiculously emotional. I don’t think of myself as a crier. As a child I learned not to cry at all costs. I rediscovered my tears when I became a mother, but in the past two years, I surprise even myself with sudden and unpredicted weepiness. I mentioned crying as I told a Starbucks barista in Barcelona how delightful it was for me, a mother of a child with Down syndrome, to see the respectful and fun relationship the café employees had with their team member who has Down syndrome. What I did not write in that essay was that every morning in Spain, every single morning, I cried. Most mornings, Claude rose and went for a run, leaving me to shower and get dressed. Before I did, however, I’d pull up Facebook on my phone while still lying in bed and weep over the pages of the babies who had died the week before I’d joined Claude in Spain. After her first heart surgery more than a year ago, Fiona’s remarkable parents created Fiona’s Hope Totes, which has its own Facebook page. This non-profit delivers care packages to families in Minneapolis/St. Paul who are experiencing an unexpectedly extended hospital stay with a sick child. The day before she died, Fiona’s family posted an urgent request for prayers as Fiona had been rushed back to the hospital due to complications after a second heart surgery. In the weeks after she died, that post requesting prayers remained the last post on the page, like a scream that wouldn’t fade as the family privately grieved.
Baby Annie’s doctors would not place her on a heart transplant list, whether due to complicating medical issues or the fact that she had Down syndrome remains ambiguous (that there is discrimination against the developmentally disabled getting organ transplants is not ambiguous, the subtle discrimination is real). Annie’s parents opened their lives to the world on her Facebook page, Annie Golden Heart. When I learned of her situation, Annie was alive, but in hospice attended by her parents and two sisters. Each day, I followed her page, hoping for a miracle, hoping as her story drew substantial attention from people worldwide that someone, somewhere would find a way to save that baby. Instead, day-by-day as I and countless others watched, Annie grew bluer, more lethargic and puffy. And then she died. In Spain, I saw the daily posts of a family submerged under and shattered by grief. Pictures of a baby’s grave more preciously decorated than any child’s bedroom, photos of a healthier Annie just months earlier including a collage of the once smiling tot with vibrant red hair and the facial features of her daddy. However, the photo that made me touch my iPhone screen with my finger, as though I could pass comfort through my device, was of Annie’s oldest sister with her face painted to look like a tiger. The caption read: Today is Nicole’s 9th bday. She has been a great sister to Annie. We are so thankful to Marie for taking the girls out today to have fun since it’s still very hard for us to even leave the house. Happy Birthday, Tiger!!!!
Only recently did I learn that baby Ryder had group B meningococcal disease, the most common strain of bacterial meningitis found in the United States (though Ryder did not live in the U.S.). I have found no evidence that having Down syndrome makes a person more susceptible to meningitis or the consequences of the disease more severe. What Ryder’s family is going through I would not wish upon anyone, but his Down syndrome had nothing to do with his death. I carried those babies, Fiona, Annie, and Ryder, with me as I traveled Spain with Claude. When we visited churches, I looked for La Pieta stations in which Mother Mary holds her dead son, Jesus, just after he’s been removed from the cross. When I found them, I lit a candle for those families. You do not have to be Christian, only human, to feel the emotions of that station in Mary’s life. It’s easy to imagine for centuries parents who have lost a child have found La Pieta a sanctuary of familiars.
When I returned to the States, I was too busy to look at Facebook for a few days. When I did, I saw that Annie’s page had been taken down and Fiona’s Hope Totes had resumed. Fiona’s valiant family was once again delivering care packages to families. Everyone’s journey with grief is unique and there is no accepted protocol except to grieve. A few days later, Annie Golden Heart was again a page on Facebook. I found Ryder’s page and his parents and two older brothers have taken Ryder’s favorite toy, Bear-Bear, traveling with them and posting photos of the white bear at an aquarium, a theme park and in the arms of Ryder’s older brother who took Bear-Bear to bed with him for comfort.
The Ones Who Live
Most babies born with heart defects survive due to surgical corrections that have, in most parts of the world, become routine procedures. But sometimes babies born with congenital heart defects, both with and without Down syndrome, die. And the parents who lose children with Down syndrome grieve every bit as much as other parents. But what about the children with Down syndrome who live? Most, but not all, babies born with Down syndrome have developmental delays. Meaning, things just take longer and sometimes more support is required along the way. Though hitting developmental milestones later than their peers without DS, most people with Down syndrome will walk, talk, dress themselves, read, go to school, graduate high school, cook, receive post-high school education or training, get jobs, fall in love, live independently, grow old and, like us all, one day die. That is “typical” life with Down syndrome. But what about the babies who face medical challenges beyond developmental delays and heart defects?A friend recently posted that she worries about telling people her son with Down syndrome has seizures. She is glad “he’s alive and he’s mine” but fears that someone else expecting a baby with Down syndrome who knows her son has seizures may chose an abortion based upon his case. Another friend told me about a woman who is a single mom of a boy with DS who is probably deaf, cannot talk, and cannot walk.
We, in first world countries, live in a medically miraculous time. A time unlike any known to humanity, in which death does not often visit us until we are middle aged. My ex-husband’s family lived for well over a hundred years in a small town in southeastern Ohio. Over the years, I heard stories of an ancestor named Flavia. Born in Germany, she studied music and had been introduced to at least one famous composer. In their tiny town in Ohio, Flavia taught music to children and had a parrot that often provided vocal accompaniment. On a visit back home (as my ex-husband used to call it), his aunt told us that Flavia’s gravestone had been vandalized and repaired. Later that afternoon, we stopped at her grave, which we had learned only that day was very near the city’s brick firehouse. I have no recollection of Flavia’s gravestone; I only remember the two stone lambs carved in marble on top of much smaller gravestones next to Flavia’s. Cholera claimed two of her children, ages four and six, in one summer, something nobody had ever mentioned. In the nineteenth century childhood death was not remarkable, yet families grieved as deeply as they do today. Visit any cemetery that dates back before the existence of antibiotics and you will find entire sections devoted to children, families who birthed eight, ten, or more children only to bury all but one or two.
Overwhelmingly, modern medicine is good, but not everything can be fixed. In the typical population, children are born regularly with, or later develop, learning disabilities, autism spectrum disorders, seizures, cancer, mental illness, vision and hearing difficulties. As of now, and unlike Down syndrome, these conditions cannot be detected with prenatal testing. However, that will likely change. And when it does, what will then be considered acceptable? Who defines which babies are perfect enough to be born? In human history, one need look no further than the past century to find pernicious programs to reduce or eliminate certain groups. Black women in the United States were frequently sterilized without their knowledge or consent. The Nazis target Jews, gypsies, homosexuals and the developmentally disabled (among many others) for systematic elimination. As the child of Christian missionaries in China, Pearl S. Buck regularly found the corpses of female newborns who had been discarded like trash. Looking back, this much is clear: once a society has decided that certain groups are not equal or good enough to exist, that decision is never static. If today it seems reasonable to seek a society free of members with Down syndrome, I guarantee that in the near future, particularly as prenatal testing begins to tease out more and more pre-existing conditions or potentials, the slippery slope of genocide will expand.
Weeding Out Variation
That Down syndrome is diagnosable, not only at birth, but also in prenatal testing, is good because, unlike autism or dyslexia, which are subjective diagnoses, results come easily and quickly. With an accurate diagnosis, appropriate support can be given to maximize the potential of an individual diagnosed with Down syndrome. However, because it is a yes-or-no clinical diagnosis, parents can also elect to abort a fetus because it has Down syndrome. Let me be transparent: I believe abortion should be safe and legal. I also believe it should be extremely rare and that support, including free birth control, should be available to all women to reduce the number of abortions. However, what the population with Down syndrome now faces is not an issue of abortion rights, but human rights. To target a specific segment of the population for elimination is simply genocide. We now have the medical means to tell a woman with a simple blood test whether or not her fetus has Down syndrome, underscoring two important points:
Making abortion illegal won’t stop the termination of pregnancies where the fetus has Down syndrome any more than it would end abortion for fetuses with 46 chromosomes. In Ireland, where abortion is illegal, the abortion rate for pregnancies where the fetus has tested positive for Down syndrome is 50%.
Once we’ve chosen as a society to decide who is human enough to live and who needs to be eliminated, watch out. Any group could be next.
Unbiased, accurate information is every woman’s right when receiving a diagnosis of Down syndrome for her fetus or newborn.
In the U.S. we know, based upon statistics, approximately how many babies should be born each year with Down syndrome. But, on average, only about half as many are. For several years in Denmark, aggressive prenatal testing accompanied by counseling that encourages aborting fetuses with Down syndrome has brought the rate of Down syndrome termination to a consistent 90%. In France, it’s over 80%.
My Child Is a Figurative Billboard
In early June, before all those sweet babies left us, my partner Max and I went to a party. We brought four of our children, Hugo, Jules, Leif and Lyra, to the family-friendly event at a beautiful home with a sprawling yard. I had a fabulous conversation with a woman who was smart and funny. After a long conversation, we separated and then reconvened. Lyra was nearby hustling around on all fours with her newly-perfected bear walk.
“She’s so cute, how she crawls on her hands and feet.”
“ Yeah, it takes them so much longer to crawl and walk with Down syndrome.”
“Wait, your daughter has Down syndrome?” the woman asked, looking astonished.
“Oh, yes,” I said. To me it is obvious Lyra has DS, but I am now firmly located on the inside of the larger community of those who have family members with DS and can recognize it more readily than I could before Lyra was born.
“You are so much stronger than I could have been,” the woman said and I disagreed with her. “No,” she continued, “I’m telling you that you are stronger than I was. In my late 30s, I was still single, I had IVF to get pregnant. When I was pretty far along, they told me the baby had Down syndrome and gave me two days to decide. I couldn’t do it. I would have been alone, I…I didn’t do it.”
“I have no judgment,” I said, knowing this woman made the best decision she could with the information she was given. I then watched the features on her face rearrange themselves, her eyes going from narrowed and intense to wide and open.
“But I see your daughter and,” she paused, “it makes me wonder.” I gave her my card, but not surprisingly, I never heard from her. In five minutes, I watched a woman think she could not have possibly raised a child with Down syndrome to wondering deeply, perhaps painfully, what her life really might have been like as the mother of a child with Down syndrome.
Educating the Gatekeepers: Medical Professionals
It is tragically ironic that at a time when we better understand Down syndrome as a range of developmental delays and that those who are diagnosed with DS often positively respond to appropriate interventions, the termination rates in pregnancies with a diagnosis of Down syndrome are escalating to an alarming degree, in some places to the point of annihilation. We have the knowledge to diagnose and remediate Down syndrome but far too often, the message given with the diagnosis over-emphasizes worst case scenarios or contains information that is ridiculously inaccurate. (See the opening quote of “Fully Human and in Need of a Civil Rights Movement.”) Medical professionals, whose job it is to know the latest research findings, are not always giving scientifically accurate and balanced accounts of what it means today to be born with Down syndrome. In fact, statistics suggest that more often the opposite is true. My own understanding of Down syndrome has dramatically changed since the birth of my daughter. What I once saw as the reality of life with Down syndrome I now realize was based upon meeting people who had spent their entire lives, often beginning at birth, in institutions. My daughter stands on the shoulders of the past two generations of people born with Down syndrome who have been raised at home and in their communities, many of whom have worked with physical therapists, occupational therapists and speech therapists. Just as with her brothers, we expect Lyra to strive, even work hard, for all she can accomplish while we support her efforts in any way we can.
Preaching Past the Choir
Parents who have children with Down syndrome know that our children are more alike than different, that they enrich our communities and deserve, as do all human beings, to live full, productive lives. However, until everyone who does not have the pleasure of knowing someone with Down syndrome is made aware of the full humanity of people with Down syndrome, the population remains at risk for a quiet campaign of prenatal genocide and medical discrimination, whether in the form of inaccurate information at diagnosis, low expectations of children with Down syndrome (she’ll walk/talk/learn poorly because she has Down syndrome), or unequal access to medical care, including organ transplants. There are a number of organizations working to eradicate discrimination against people with Down syndrome by educating people everywhere. Please feel free to share the names of organizations you know of in your comments. Here are some that are doing very important work:
The National Down Syndrome Congress: These are the folks who conduct the annual convention we have attended each year since Lyra’s birth have as their campaign “More Alike than Different.” Their mission is “provide information, advocacy and support concerning all aspects of life for individuals with Down syndrome, and work to create a national climate in which all people will recognize and embrace the value and dignity of people with Down syndrome.”
The National Down Syndrome Society: With the mission “to be the national advocate for the value, acceptance and inclusion of people with Down syndrome,” NDSS often takes the lead on legislative issues such as the ABLE Act (read about the ABLE Act in “Miss Lyra Goes to Washington“). NDSS is the national sponsor of the Buddy Walk, a fundraising and awareness campaign that takes place each year in cities across the United States. Our local support group, The Upside of Downs, is an affiliate of NDSS.
Down Syndrome Diagnosis Network: This newly formed organization was created by a group of Mamas who have babies the same age as Lyra. DSDN’s long-term goals include filling in the gaps of inadequate support systems. In addition to supporting new families, DSDN is focused on changing the diagnosis conversation with the vital mission to help “parents give their medical providers feedback on the quality of their prenatal or birth diagnosis conversation. DSDN provides health professionals the necessary resources in order to deliver future diagnoses with unbiased information and support.” Read: gatekeeper education campaign. The work of DSDN is paramount, now more than ever.
The National Center for Prenatal and Postnatal Down Syndrome Resources: Complementing the work of DSDN, this organization is a clearinghouse of the most up-to-date information regarding Down syndrome. Furthermore and significantly, this organization tirelessly advocates for legislation, state-by-state, requiring accurate information be given with a diagnosis of Down syndrome. For information on the various states that have passed legislation requiring accurate information to accompany a DS diagnosis, and how it has been carried out, read this.
The National Down Syndrome Adoption Network: Not everyone, for whatever reason, can raise a child with Down syndrome, like the single mother who struggles to raise her son who is also medically fragile. And no matter how much education is given, there will still be some families who simply may not want to keep a child with Down syndrome. NDSAN is a non-profit that works both with birth families seeking placement of a child with Down syndrome and families who wish to adopt a child with Down syndrome with the mission of ensuring “that every child born with Down syndrome has the opportunity to grow up in a loving family.”
The Choices People Make
Along with the families who lost their babies this summer, I have thought frequently about the woman I met at the party who had terminated her pregnancy. Her desire for a baby had to be substantial as IVF is a painful, lengthy and expensive process. But then she was given frightening information and the directive to decide in two days what she would do. Knowing what I know now, I can only wonder: What if she had met Lyra before she received the diagnosis? What if she—and thousands of expectant mothers like her—had been given accurate information along with resources for support? I cannot help but believe, based upon the change I saw this woman undergo in five minutes, that today she would be the proud mother of a child with Down syndrome. And if all women were to receive the full and unbiased information that they deserve as autonomous adults, would we then be closer to a society that values the human rights of its Down syndrome citizens, rather than one that tacitly endorses the elimination of that population? I believe that, yes, we would.
Our home has been temporarily rearranged. The water bowl for the dogs and cats is now commonly found on the kitchen counter while the bathroom trash cans currently reside atop the closed lids of the toilets. A paper grocery bag containing paper recycling was handily located in the kitchen. Lately it can be found a few feet away in a lower level vestibule, which is inaccessible to the littlest resident of our home who knows how to climb up, but not down, stairs. She mastered stair ascension when she discovered the bin of bath toys hidden in the empty tub, alongside of which is a single step.
Lyra, our curious baby, is on the move and eager to exercise her self-determined mission: find all containers, empty them of their contents and, before spreading said contents far and wide, taste as many of them as possible. Hence, the reorganization of our home, something I have had to do four times before when each of my boys were curious and accomplished crawlers. She may be older than they were at this stage, but she doesn’t look it. Furthermore, her mind works just as theirs did—once a container full of clean diapers or dirty trash, toys or recycling (all equally appealing it seems), has been discovered, the site is frequently revisited.
From my earliest conception of Whoopsie Piggle, I planned to write about our entire family and not just our youngest child, Lyra, and her diagnosis of Down syndrome because her diagnosis neither defines who she is as a person nor who we are as a family. Yes, her diagnosis helps us to understand her needs in order to better meet them, just as the diagnoses of dyslexia helped us to meet the needs of her older brothers, Claude and Jules. In fact, in the past few months it has been harder to write essays isolating the latest in Lyra’s life. On occasion we have bigger issues to address, but most days are entirely mundane and typical of any household with a crawling baby. Lyra is no longer brand new. She exhibits a fully formed personality with many things that make her giggle (her brother Leif, getting tossed in the air, singing to the pretty baby in the mirror, kisses on her neck) and others that make her howl (diaper changes, bedtime, hunger, blood draws, contact lens changes). Lyra is an integrated and integral member of our family. Certainly she has made great developmental strides thus far this year and yet this fact makes her seem all the more typical and her accomplishments less, not more, noteworthy.
A Babyhood of Appointments
The first few years of life for a child with Down syndrome often require regular interventions in order to acquire well-developed gross motor skills (sitting up, crawling, walking, running) and fine motor skills (i.e., purposeful hand skills such as self-feeding), and speech. The common culprit underlying these delays is not necessarily a cognitive issue, but hypotonia, or low muscle tone, which affects almost all babies with Down syndrome. In talking with parents of older children with DS, including adult children, many recall the constant work in the early years of their child’s life. Since she was three months old, Lyra has had regular therapies (speech, physical and occupational). For the last six months, she has gone twice a month to Akron Children’s Hospital for what they call an “infant block” in which all three of her therapies are conducted back-to-back by a team of therapists who discuss and coordinate her care.
When older children and adults receive therapies, as many people do after an injury or medical event, the therapist trains the individual. But when the client is a baby, the therapists train the caregivers more than the client. Yes, Lyra recognizes her therapists and knows her way around the room where they conduct her appointments. But to Lyra therapy must seem like a play date. The occupational therapist blows soap bubbles for Lyra to pop with her forefinger, the speech therapist looks into a mirror with Lyra as together they sing songs and practice sounds, and the physical therapist pulls out toys that engage Lyra so deeply she doesn’t notice she had to climb a small hill or stand up on her own to reach whatever bright, noisy (and oh-so-non-Waldorf) plaything the therapist uses as bait. And then we try to replicate it all at home.
Meanwhile, back at home, Lyra is also visited by her Summit County Developmental Disability Board caseworker and her Cleveland Sight Center caseworker, both of whom observe her progress and also make recommendations, generally taking into account our home environment. For example, instead of buying an expensive Little Tikes climbing wall, as Lyra’s pediatrician had urged, they helped me arrange the tumbling mat we own over some pillows, which Lyra now repeatedly climbs up and over.
Sometimes the folks coming to our home tell us the very same thing I hear at the hospital. Other times, they do not. For example, after Army-crawling for three months, Lyra began crawling on her hands and knees and soon thereafter she started what we call “bear-walking,” or walking on her hands and feet. And even though it has given Lyra a speed and facility at dumping out trash, recycling, toys and whatever else she can find, we have been rooting her on. It’s thrilling to see her motor around and the hospital’s physical therapist agreed. Her caseworkers were less excited. Sure, it’s great that she’s getting stronger and moving. But her back legs were being held too far apart, like an upside down wide V, putting pressure on her hip sockets. Along with hypotonia, people with Down syndrome commonly have ligament laxity and by stressing the exterior of her hip sockets, the caseworkers explained, Lyra can wear down her ligaments thereby opening the door for a host of other issues, including chronic pain.
The solution? Hip Helpers. We used these many months ago, when Lyra was learning to sit up on her own, but they were all but moth-balled since Lyra took off Army-crawling in January. Like a pair of tight spandex shorts, Lyra’s daycare provider and I both refer to them as Lyra’s “Spanx,” the modern day equivalent of a girdle. Hugo calls them Lyra’s “mermaid thingies” as they keep her thighs together like a big fish tail. Under her dresses and skirts, Lyra’s Hip Helpers look like baby shorts, stylish even. With them on, however, she cannot zip around as easily. For now, that is. The goal is to retrain Lyra’s legs to move correctly, and not splayed out, as she ambulates, something she is highly motivated to do (so many trash/toy/recycling bins, so little time).
For two weeks, Lyra wore her Hip Helpers all day, every day. Then we had our next Infant Block appointment at the hospital where the physical therapist pointed out that Lyra locked her knees more when wearing the Hip Helpers. Also important, the hospital therapist questioned making Lyra struggle with a skill she had just acquired (bear crawling). And so, we agreed upon the middle path (or the Buddhist take on pretty much everything)–not too much, not too little and, as of this week, our busy monkey spends about half her days in her Hip Helpers.
Seat Swiveling
Here Comes that Girl
Bear Crawling
Speaking with a Star
I just saw an adult with DS at the movie theater and I wanted to run up and hug him. It was like a celebrity sighting LOL. Is that just me?
~A post on a Facebook group for mothers with babies born in 2012 and 2013 and diagnosed with Down syndrome.
Comedian Rob Snow and his wife, Ellen, who live in Northeast Ohio, founded the non-profit organization, Stand Up For Downs. In his routine titled, “We Need a Sign,” Snow describes a walk he took shortly after his son Henry was born with Down syndrome. When Snow saw a family of children running and playing in their yard, including a girl with Down syndrome, he was momentarily riveted as he watched the girl doing and being everything any other child her age would do or be. When the children ran off, Snow noticed a woman, presumably the girl’s mother, looking at him with irritation, if not outright anger. She thought he was a rude gawker. The moment was awkward and Snow quickly walked away without explaining that he had a newborn son with Down syndrome. We need a sign to let one another know, “Yeah, me too, my child has Down syndrome.”
I laughed throughout most of Snow’s routine at a new parent event sponsored by our local support group when Lyra was only a couple of months old. But as he described staring at the girl and not finding a way to talk with her mother, color rose up my neck and my ears became hot with embarrassment. When Lyra was perhaps a week or two old, we had taken her and the boys to Five Guys Burgers for lunch. Asleep in her car seat, Jules sat with Lyra at a table while the rest of us got in line. Behind us, but separated by another group of people, was a family that reverse-mirrored our own—instead of four boys and a baby girl, they had several daughters and little son, who appeared to be about Leif’s age, which was two-and-a-half at the time. Leif and the little boy pushed the red cordon, hung between posts to form an orderly queue at the restaurant, with their hands to make it swing back and forth. The two little boys were twin-like–they stood at the same height, had equally white-blonde hair, and deep blue eyes. But the other little boy’s eyes had the characteristic shape associated with Down syndrome. Staring does not describe my behavior. I scrutinized the child, who had on a red zip-up hoodie from the Gap and blue jeans, an outfit nearly identical to Leif’s, and only tore my eyes away to shyly smile at the child’s father, a big man with a beard who smiled in return. I wanted desperately to tell him and his wife that my new baby had been diagnosed with Down syndrome but I was uncharacteristically struck speechless.
In the first few months after Lyra was born and we learned she has Down syndrome, I regularly wondered how having an extra chromosome would effect Lyra. Would she talk? Would I be able to understand her? Would she develop like other children or would she be a perpetual infant? I did not know and nobody could tell us. Sighting an older child, even one who was only two or three years old, when Lyra’s life had just begun, loosened my mind’s grip on my worst fears by showing me: This too is possible, a child more alike than different.
Last weekend, we were seated in the waiting room of the lab at Akron Children’s Hospital where we take Lyra quarterly to have her blood drawn for a thyroid level check. A woman and teenaged girl with Down syndrome walked in and I (rudely) listened to the mother give her daughter’s date of birth to the receptionist. The girl had recently turned fourteen, which makes her only a couple of months older than our son Jules. With Lyra in my lap, the mother and daughter began talking to us before they sat down.
“She loves babies,” said the mother.
“Yes, I do!” said the daughter.
When the phlebotomist called for Lyra, Max took her back while I stayed and talked with the two women, and a pattern I’ve now seen many times emerged: the daughter spoke and then the mother repeated and/or clarified what her daughter said.
Me: I love your nail polish.
Girl: My mom did my toes, but I did my hands.
Mom: I did her feet, but she did her fingers, well, most of them I see. She’s so independent; she tells me all the time, I’ll do it myself!
Me: What grade are you in?
Girl: Seventh grade. I love school, I’m a cheerleader.
Mom: She’s in the seventh grade; it’s a great school. They have a cheerleading squad called the “Sparkles.”
Girl: Yes, I’m a cheerleader.
Mom: She’s like a rock star at her school, seriously.
We stopped talking when Max brought out a sobbing Lyra with both elbows wrapped in Day-Glo pink cling tape, used these days instead of Band-aids to hold a gauze compress at the site of the blood draw. They had not been able to get a sample of Lyra’s blood and Max described a scene I’ve witnessed all too often in which the phlebotomist sticks Lyra’s arm with the needle but cannot find the vein and begins grinding the needle around in her arm in an attempt to locate the vein. We were told to bring her back on another day for another round of this torture.
As I begin comfort-nursing Lyra, the girl I had been talking with was called back for her blood draw and in what seems like less than a minute, she’s back out, tear-free.
“Wow, that was fast!” I told her.
“Yeah, I’m a big girl,” she said and Max slapped her a high-five.
Right Before Our Eyes—What We Did Not Know
“20/270, that eye is legally blind and 20/180, that eye is what they call ‘legally visually impaired’ but any school district would categorize her as legally blind,” said Lyra’s vision specialist.
“That’s with her contact lenses in?”
“Oh, yes. Without the contacts—well, she has no lenses inside her eyes, as you know, and without the contacts, it would be much worse.”
“But how can this be? Every time we see the ophthalmologist, he tells us her eyes look great and that he couldn’t be more pleased. And she sees us, the things she plays with. I mean, she certainly moves from one side of the kitchen to the other to get to the bag of paper recycling. Is it just that she remembers that it’s there?”
“Well, certainly her memory is helping play a role in how she uses her vision. This is a very non-medical explanation, but imagine what you see at 270 feet, she would need to be only 20 feet away to see the same thing. And I like to tell my parents that it is like a big funnel. Right now, Lyra is looking at the big world around her, but as she begins to focus on holding a crayon, writing, reading—really narrowing her field of vision for specific tasks, her visual limitations will become more apparent.”
I paused and thought of something I had long noticed: when Lyra is in my arms, her eyes are wide open, big and blue and often staring into my own. But when she is more than a couple feet away, she squints. I have a hard time capturing her in photos without her squinting, but usually when I am taking her picture, I am more than a couple of feet away. Just as when I try to read the clock in the morning without first putting on my glasses, Lyra squints in an effort to see more clearly.
“So what I want from you now,” I said, my voice becoming husky as I grabbed a tissue to mop the tears suddenly springing out from behind my glasses, “is for you to look into your crystal ball. Like, does this mean she’ll walk with a cane?”
“Well, first of all, I think her left eye is already better than when this last test was taken. And we have until she is about age five or six for her eyes to improve. Now when she starts walking, she’ll probably have glasses as well as her contacts because she’ll need the glasses to give her the ability to see in the distance, like a bifocal.”
“Okay.”
“But it’s good she’s crawling for so long because she is learning where all the bumps are in your floors.”
“Wow, so I guess we can never move from this house.”
“Nope,” said the vision specialist and smiling playfully she added, “Nor can you ever move the furniture.”
“So what about when she’s out? She will need a cane then?” The notion of Lyra walking with a cane suddenly became emblematic of everything I feared about her being blind: With just a glance, anyone would recognize her two disabilities for which she may be unfairly assessed as not capable of any number of things she deserves, including employment, housing, and civility.
“Well, I can’t say for sure, but I don’t think so. However, we will teach her techniques, such as sliding the outside of her hand, with her fingers cupped so they don’t get caught behind things like fire extinguishers, alongside the wall of a room she’s unfamiliar with so she’ll not run into things.”
“Ahh,” I say as it all starts to click.
All We Can Handle
I’ve long known that Lyra’s ophthalmologist does not like to talk about Lyra’s vision, or about what procedures, or outcomes to anticipate. I know this because he’s told me as much. I chalk it up to needing to wait and see how Lyra develops. If she does great with contact lenses, stick with contacts and avoid more surgery. At her strabismus surgeries last summer, her ophthalmologist told us that as she got older he would be able to put her in different, less bulbous, contact lenses. Her vision was corrected for the world of a baby, roughly up to two feet away, but he said that he’d change her correction as she got older and began walking.
Because of these conversations, we believed all along that Lyra was seeing, well normally, like most any other baby. Instead she’s legally blind. I only worried about it when another mother wrote to me, a woman I do not know but who recently was put in touch with me by a mutual friend. This woman’s son, who is a few months younger than Lyra, was also born with bilateral cataracts and now sees at 20/60 and 20/90 and she was worried about what his future would be like. I wrote and told this mother what we are doing for Lyra but never heard from her again and I wonder if it isn’t because Lyra’s vision is substantially worse than her son’s vision. Her letter inspired me to call Lyra’s vision specialist and ask her to sit down and tell me what a vision acuity score of 20/180 and 20/270 mean for Lyra long term.
I imagine had the ophthalmologist told me in detail at Lyra’s first surgeries, more than a year and a half ago, what we would be facing when she was older, it would have overwhelmed me or, at the least, been so much information on top of the information we needed in the immediate moment, that I would have forgotten much of what he said. To be honest, perhaps he did tell us much of what we now need to consider and it did slip into the cracks of my overloaded brain.
Climbing mountains, no matter how high, happens one step at a time.
Normal Is As Normal Does
Lyra will turn two in August. She talks, uses sign language, plays with her brothers and her daycare friends, sings songs, makes animal sounds on her own and when asked, crawls, “sorts” laundry, pats my back just as I pat hers, just as all my babies often patted my back when held up to my shoulder because that is what I do to them. Lyra’s daycare provider could not love Lyra more if she were her biological niece. Everyday of her life, everywhere she goes, Lyra is encouraged to move her body in ways that will protect her health long-term, and avoid issues such as displaced hips and pronated feet.
We did not anticipate how musical Lyra would be when we gave her a name related to the word “lyrical.” Perhaps the name was providentially chosen for nothing pleases Lyra more than singing. Much of her speech has developed through song, she is calmed by song when sad and I even use it as part of my arsenal to distract her when need be. Placing her in front of the mirror on my dresser, Lyra and I sing together while pulling her hair back into a ponytail, something she otherwise resists.
For several weeks, Lyra’s team, including everyone in the family, her therapists and her daycare provider have talked about how it’s coming together beautifully for Lyra and all the progress she has made and continues to make. At Akron Children’s Hospital, the therapists tell me, each and every visit, what a thrill it is for them to see what new things Lyra has learned since her previous visit.
Learning Lyra is legally blind was not devastating, but to use a cliché, I felt the wind drop from the sails of all that wonderful momentum in Lyra’s development. This too? Isn’t Down syndrome enough? But that is me feeling sorry mostly for me and not Lyra who, after all, only knows what she knows. For her, life is full of loving people and good times. She’s as happy as a baby should be and not moping about because she has to work harder to crawl and can’t see as well as anyone else she knows. Again, for now at least, she isn’t aware of any differences. Who knows how she’ll feel one day when she does realize how her life is different? My personal experience now having met so many people of all ages with Down syndrome, as well as the scientific research, gives me every reason to believe Lyra will be happy with who she is.
So we breathe in, breathe out and pick up the phone. First call: The ophthalmologist to learn what we can do to improve Lyra’s vision before she turns five years old. Second call: The vision specialist to learn what compensatory techniques Lyra can begin learning now.
And, as with all things, our journey continues. One step at a time.